



Original Article - Year 2013 - Volume 28 -
Syndactyly after hand burn
Sindactilia pós-queimadura da mão
ABSTRACT
INTRODUCTION: Syndactyly caused by burns to the hand is a severe and disabling sequel that limits hand function. In most cases, it results from poor scar orientation during the acute phase of the burn. This article describes the systematic technique adopted by our institution to treat this sequel, and establishes normal parameters to be investigated and surgical techniques.
METHODS: Between January 2009 and December 2012, 150 patients with syndactyly caused by burns to the hand underwent reconstructive surgery. The following 4 surgical steps were used to treat all patients: preparation of the dorsal flap; syndactyly release; migration and suturing of the flap to its new position; and skin graft to fill the remaining spaces.
RESULTS: There was graft survival in 100% of cases. Partial graft loss occurred 20 cases, and there were no cases of local infection. All patients recovered their hand function, including the ability to hold, and digital abduction.
CONCLUSIONS: Syndactyly after burns is extremely limiting to the patient. The use of basic techniques of flaps and grafts results in successful treatment, restoring hand function compromised by the injury.
Keywords: Burns/complications. Burns/rehabilitation. Hand. Syndactyly/surgery.
RESUMO
INTRODUÇÃO: A sindactilia por queimadura é uma sequela grave e incapacitante, e limita a função preensora da mão. Na maioria dos casos, é decorrente de má orientação cicatricial na fase aguda da queimadura. O objetivo deste artigo é descrever sistematização técnica adotada em nossa instituição, estabelecendo parâmetros de normalidade a serem buscados e técnicas cirúrgicas que auxiliem no tratamento.
MÉTODO: No período de janeiro de 2009 a dezembro de 2012, 150 pacientes portadores de sindactilia decorrente de queimadura da mão foram submetidos a cirurgia reparadora. Em todos os pacientes, foram adotadas 4 etapas cirúrgicas: confecção do retalho dorsal; liberação da sindactilia; migração e sutura do retalho dorsal para sua nova posição interdigital; enxertia dos gaps com pele total, preenchendo os espaços remanescentes.
RESULTADOS: Em 100% dos casos houve total sobrevivência dos retalhos, com perda parcial de enxerto em 20 pacientes e nenhum caso de infecção local. Em todos os pacientes dessa série foi observada recuperação da função da mão, com capacidade de preensão e de abdução digital restauradas.
CONCLUSÕES: A sindactilia pós-queimadura é uma deformidade extremamente limitante ao paciente. O emprego de técnicas básicas de retalhos e enxertos proporcionou sucesso no tratamento, com restauração da função da mão, comprometida pela lesão.
Palavras-chave: Queimaduras/complicações. Queimaduras/reabilitação. Mãos. Sindactilia/cirurgia.
The hand plays important roles in human labor and relationships. During sensory and motor activities, the hand is the most prone to accidents among body parts. Therefore, the hand may be the part of the body most affected by burns1.
Burns should be treated as early as possible, because the recovery time is a crucial factor for functional recovery and the incidence of sequelae.
Syndactyly caused by burns is a severe and disabling sequel that limits hand function. In most cases, it results from poor scar orientation in the acute phase of the burn. The plastic surgeon should understand the functionality of the hand to correctly treat the syndactyly 2-4.
There are many reported treatments for this sequel with various features and behaviors 5-8. We have adopted a systematic technique at our institution that optimizes results and improves the function of the hand. This article describes this systematized technique, and establishes normal parameters to be investigated and surgical techniques that aid the treatment of this sequel.
METHODS
Between January 2009 and December 2012, 150 patients with syndactyly caused by burns to the hand underwent reconstructive surgery.
All patients underwent the same surgical approach, which involved the following 4 sequential surgical steps:
1. The dorsal flap is prepared. Rectangular flaps in the dorsal region of the hand are marked with methylene blue, and incised and raised from their bed.
2. The syndactyly is released by removing the interdigital scar retraction until complete abduction of the fingers.
3. The dorsal flap is migrated to its new interdigital position and is sutured to the edge of the palm of the hand.
4. After the previous steps are completed, "gaps" remain in the lateral margins of the flap, because it does not have enough skin to completely cover the raw areas that emerge after syndactyly opening. At this time, grafting is performed with total skin, filling the remaining spaces.
RESULTS
Flap survival occurred in all 150 cases in which the systematic surgical approach described above was performed. Partial graft loss not requiring re-grafting occurred in 20 cases. There were no cases of wound infection.
All patients in the present series recovered their hand function, including the ability to hold, and digital abduction.
Figures 1 to 5 systematically show the procedure in 1 selected case to demonstrate the technique.

Figure 1 - Patient with post-burn syndactyly for 5 years. There is no skin in the dorsal region due to burn scar retraction with the deletion of interdigital commissures, change in nail edge, and limited abduction of the fingers.

Figure 2 - Dorsal flap marked on the second and third interdigital spaces between the ring and little fingers, delimiting Z-plasty.
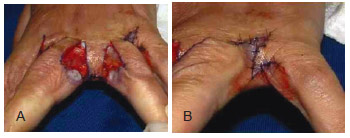
Figure 3 - In A, a large gap that presented with the opening of the commissures. It is evident that the dorsal flap is unable to cover the entire area when performing normal abduction of the fingers. In B, aspect of the fourth interdigital space with only the corrected Z-plasty, enabling full abduction.

Figure 4 - In A and B, postoperative appearance after the final positioning and suturing of skin grafts (taken from the anterior fold of the wrist or the groin) prepared and honed with scissors).

Figure 5 - Appearance 12 months postoperatively, showing complete restoration of the commissures and digital correction of the retractions, which were determined by the lack of skin on the back. Complete abduction of the fingers and hand pressing capacity were restored without limitations. Aesthetic improvement of the hand after the correction of skin retraction in the nail region can be observed.
DISCUSSION
The treatment of syndactyly as a burn sequel follows the same principles as those for congenital syndactyly, except that in the former, all commissures are treated in a single surgery only.
Another important point to be considered is that the sequel is caused by burning and therefore arises from a lack of skin. Thus, flap formation followed by grafting is mandatory because this sequel is impossible to treat with flaps only.
Browne et al.7 describe a technical approach using flaps and grafts for severe contractures and Z-plasty for the simplest cases. The same practice has been adopted at our institution.
Even though the skin area to be operated on had poor quality as it was healing from a burn, flap survival was observed in all cases. This highlights the fact that the flap is the most important part of this surgery. The graft did not fully attach in 20 cases, possibly due to excessive finger movement or a layer of blood between the graft and its bed. There were no cases of infection even though no antibiotics were prescribed postoperatively.
It is worth nothing that patients who have not yet reached adulthood may require multiple surgeries to facilitate normal hand development, because the skin of burn scars does not grow in the same proportions as the surrounding healthy skin.
The use of dermal matrix for the treatment of burn sequelae in the hand does not appear to be justified, because the results with the technique presented here were very satisfactory and all patients received free treatment, which would be impossible if we used such costly products in our service.
CONCLUSIONS
Syndactyly after burn is an extremely limiting sequel. The use of basic techniques of flaps and grafts provides successful treatment, restoring hand function compromised by burning.
REFERENCES
1. Lima Jr EM, Novaes FN, Piccolo NS, Serra MCVF. Tratado de queimaduras no paciente agudo. São Paulo: Atheneu; 2008.
2. Mélega JM. Cirurgia plástica: fundamentos e arte. Rio de Janeiro: Medsi; 2002.
3. Mélega JM, Viterbo F, Mendes FH. Cirurgia plástica: os princípios e a atualidade. Rio de Janeiro: Guanabara Koogan; 2011.
4. Carreirão S, Carneiro Jr LV. Cirurgia plástica: para formação do especialista. São Paulo: Atheneu; 2011.
5. Adamson JE, Crawford HH, Horton CE, Brown LH. Treatment of dorsal burn adduction contracture of the hand. Plast Reconstr Surg. 1968;42(4):355-9.
6. Bauer TB, Tondra JM, Trusler HM. Technical modification in repair of syndactylism. Plast Reconstr Surg. 1956;17(5):385-92.
7. Browne EZ Jr, Teague MA, Snyder CC. Burn syndactyly. Plast Reconstr Surg. 1978;62(1):92-5.
8. MacDougal B, Wray RC Jr, Weeks PM. Lateral-volar finger flap for the treatment of burns syndactyly. Plast Reconstr Surg. 1976;57(2):167-71.
1. Plastic surgeon, full member of the Sociedade Brasileira de Cirurgia Plástica/Brazilian Society of Plastic Surgery, assistant professor and private practice, Rio de Janeiro, RJ, Brazil
2. General surgeon, graduate student of the Department of Plastic Surgery, New University of Iguaçu, Plastics Hospital, Rio de Janeiro, RJ, Brazil
Correspondence to:
Luiz Mário Bonfatti Ribeiro
Hospital da Plástica
Rua Sorocaba, 552 - Botafogo
Rio de Janeiro, RJ, Brazil - CEP 22271-110
E-mail: lmbonfatti@uol.com.br
Submitted to SGP (Sistema de Gestão de Publicações/Manager Publications System) of RBCP (Revista Brasileira de Cirurgia Plástica/Brazilian Journal of Plastic Surgery).
Article received: January 10, 2013
Article accepted: March 5, 2013
This study was performed at the Plastic Surgery Service of the New University of Iguaçu, Plastics Hospital, Rio de Janeiro, RJ, Brazil.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket