



Original Article - Year 2026 - Volume 41Issue 1
Low-Cost Synthetic Model for Liposuction Training and Simulation
Modelo sintético de baixo custo para treinamento e simulação de lipoaspiração
Marina Luz Zonari1 ; Leticia Timbó Martins Ferreira1; Ivens Rafael Resplande de Sá1,; José Lucas Vieira Lopes1; Artur Diógenes Vasques Farias1; Larissa Cruz de Souza1; Eduarda Maia Lima1; Victor Luis Almeida Pires de Castro1
; Leticia Timbó Martins Ferreira1; Ivens Rafael Resplande de Sá1,; José Lucas Vieira Lopes1; Artur Diógenes Vasques Farias1; Larissa Cruz de Souza1; Eduarda Maia Lima1; Victor Luis Almeida Pires de Castro1
ABSTRACT
Introduction Liposuction is a widely-used technique for body contouring and the treatment of lipodystrophies. It is one of the most performed procedures in plastic surgery in the United States and Brazil. Despite its popularity, the technique requires specific skills. As such, surgical simulations are fundamental to training doctors in a safe, low-cost environment, especially considering the gaps in traditional education and specialized training.
Materials and Methods The development of the synthetic model for liposuction training required a plastic chest mannequin, foam sheets, mesh fabric, zippers, and Styrofoam microbeads. We also used a copper air-conditioning tube to replicate the liposuction cannula, connecting it to a domestic vacuum cleaner with an adapted tube. The plastic surgeon advisor from the Plastic Surgery League of Universidade de Fortaleza approved the model and recommended it for the low-cost simulation.
Results The model presented satisfactory results in the simulation of a liposuction procedure, enabling the practice of fundamental movements, such as fan suction, and it offered a realistic, hands-on experience for the students. Furthermore, the reuse of the model and the simplicity of its materials made training accessible, promoting greater inclusion in surgical learning.
Conclusion The synthetic liposuction model proved to be an effective, accessible, and low-cost tool for the practical training of future surgeons. It provides a solid foundation for technical learning, democratizes access to surgical education, and promotes the development of essential skills, preparing professionals for real clinical scenarios.
Keywords: education, medical; lipectomy; models, anatomic; plastic surgery procedures; low-cost technology
RESUMO
Introdução A lipoaspiração é uma técnica amplamente utilizada para o contorno corporal e o tratamento de lipodistrofias, e é umdos procedimentosmais realizados em cirurgia plástica nos Estados Unidos e no Brasil. Apesar de sua popularidade, a técnica requer habilidades específicas, e destaca-se a importância de simulações cirúrgicas para capacitar os médicos em um ambiente seguro e de baixo custo, especialmente diante das lacunas no ensino tradicional e no treinamento especializado.
Materiais e Métodos Para a construção do modelo sintético para o treinamento de lipoaspiração, foram necessários um manequim torácico de plástico, lâminas de espuma, tecido de malha, zíper e micropérolas de isopor. Além disso, foi utilizado tubo de cobre de ar-condicionado para replicar o funcionamento da cânula de lipoaspiração, conectado a um aspirador doméstico por meio de um tubo adaptado. Omodelo foi aprovado pelo cirurgião plástico orientador da Liga de Cirurgia Plástica da Universidade de Fortaleza, sendo recomendado para simulação de baixo custo.
Resultados O modelo apresentou resultados satisfatórios na simulação da técnica de lipoaspiração, permitiu a prática de movimentos fundamentais, como a aspiração em leque, e ofereceu uma experiência prática realista para os estudantes. Ademais, a reutilização do modelo e a simplicidade dos materiais empregados tornaram o treinamento acessível, o que promove maior inclusão no aprendizado cirúrgico.
Conclusão O modelo sintético de lipoaspiração demonstrou ser uma ferramenta eficaz, acessível e de baixo custo para o treinamento prático de cirurgiões em formação. Ele proporciona uma base sólida para o aprendizado técnico, democratiza o acesso ao ensino cirúrgico e promove o desenvolvimento de habilidades essenciais, pois preparando os profissionais para cenários clínicos reais.
Palavras-chave: educação médica; lipectomia; modelos anatômicos; procedimentos de cirurgia plástica; tecnologia de baixo custo
Introduction
In 1983, French surgeon Dr. Yves-Gerard Illouz introduced liposuction using cannulas, sparking interest among special-ized surgeons and patients seeking body-contouring proce-dures.1 A few years later, in 1986, Pierre Fournier2 established the concept of liposuction using syringes. Since then, several technologies have emerged to facilitate the procedure, in-cluding vacuum aspiration, laser-assisted aspiration, vibroli-posuction, and, more recently, ultrasound-based technology.3
Liposuction is widely used to treat lipodystrophy and provide patients with their desired silhouette. It can treat several body areas, such as the face, neck, breasts, and flanks, although its application is most prevalent in the abdominal region.4 Today, liposuction is the most frequently performed plastic surgery procedure in the United States, and, in recent years, it has experienced an exponential growth in Brazil.5
The surgical technique involves aspirating fat using blunt cannulas that exert negative pressure on the subcutaneous adipose tissue. During liposuction, the surgeon inserts the cannula into a deep plane and, with their dominant hand, performs movements from the deeper to the superficial planes according to the amount of fat to be removed. The opposite hand remains outside the patient’s skin, monitoring the area under aspiration to guide the surgeon regarding the depth of the cannula and the amount of remaining fat.6
Although liposuction alone causes few complications, the main ones include hematomas, seromas, irregular contours, and hyperpigmentation.7 Therefore, liposuction requires skill, esthetic vision, and practice to deliver a satisfactory, harmo-nious, and safe outcome. Obtaining good outcomes requires extensive skill training by the surgical team. Several factors, including increased patient expectations, trainee schedule restrictions, and the popularization of less invasive techni-ques, have reduced opportunities for traditional surgical teaching. This scarcity revealed a gap in medical education for training in more specialized practices, leading many doctors to learn the procedure only during residency.8,9
In this scenario, surgical simulation training enables skill development and improvement in a controlled, safe envi-ronment, contributing to the progressive increase in studies on the creation of surgical models. However, limitations, such as the high cost of these simulators, have stimulated the development of equally-effective and low-cost alternatives.9
Low-cost simulators contribute to improving the skills of medical students, interns, and residents in plastic surgery. The use of models integrates theoretical learning with surgical practice in an environment designed to enable repetition and supervised by senior professionals, with no risk of harming an actual patient.10-14 Simulators are especially valuable for plastic surgery because this field presents few opportunities to train in highly-specialized procedures.
The intended use of this model is simulation in initial teaching; after all, actual procedures are under the respon-sibility of specialists and supervised residents. The reference to medical students and interns is limited to anatomical understanding, ergonomics, and step-by-step technical pro-cedures in a simulated environment. The simulator does not encourage the performance of liposuction by non-specialists.
Objectives
The present article aims to describe the construction of a novel synthetic model for training in liposuction surgical techniques, designed for ease of execution and low cost.
Materials and Methods
The current study was conducted from January to Septem-ber 2024 by students from the Academic League of Plastic Surgery (Liga Acadêmica de Cirurgia Plástica, LICIP, in Portu-guese) of the Medicine Program at Universidade de Fortaleza (UNIFOR). The team also developed a liposuction simulator, which was subsequently tested by the students and the supervising plastic surgeon.
Building the model required the following materials: 1 plastic thoracic mannequin, foam sheets (0.5 cm and 0.25 cm thick), 1.5 m of beige mesh fabric, 0.5 m of light pink mesh fabric, a zipper, and Styrofoam microbeads.
Initially, the mannequin was covered with a 0.5-cm layer of sponge, representing the subcutaneous tissue, and a 0.25-cm layer to enhance the body contours (►Fig. 1A). The team fixed these layers to the mannequin with hot glue. Next, the model received a sewn-on mesh fabric cover to give it the shape of a human bust (►Fig. 1B).
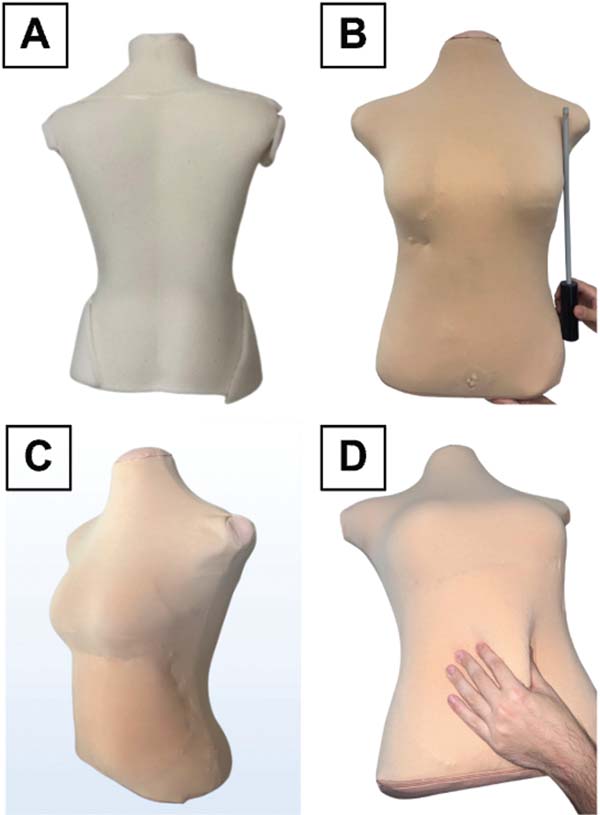

Then, the team created a virtual cavity in the mannequin’s abdominal region by applying an additional layer of mesh filled with Styrofoam microbeads and closed with a zipper (►Fig. 1C,D). This cavity enabled\ the simulation of subcuta-neous fat removal during aspiration. The umbilical region has a replaceable structure, which ensures the reuse of the simulator by creating new incisions.
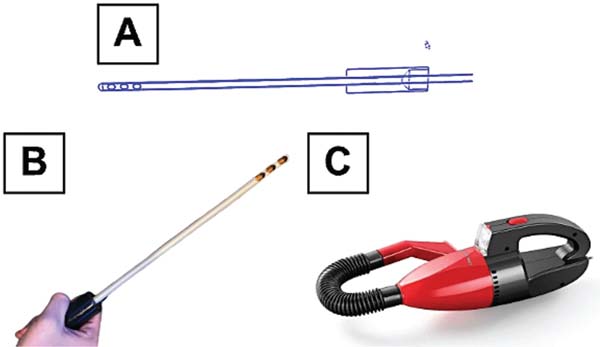
Lastly, to replicate the functioning of the liposuction cannula, the team used a copper air-conditioning tube with three holes drilled in its distal portion. This tube was attached to a plastic cylinder for connection to the suction tube of a regular household vacuum cleaner (►Fig. 2), en-abling the aspiration of the microbeads during the simulated procedure. Then, the application of paints specifically designed for these materials aimed to obtain a simulator with an esthetically-pleasing appearance.

The final production cost of the model was of R$ 261.75 (roughly less than US$ 50 in November 2025), with each simulation costing R$ 5.57. ►Table 1 shows the cost and function of the materials.
| Material | Amount | Cost | Simulated structure and/or use |
|---|---|---|---|
| Female mannequin (; ; and depth: 24 cm) | 1 unit | R$ 40.00 | Thorax þ abdomen |
| Hot glue gun (20 W) | 1 unit | R$ 12.50 | Hot glue handling |
| Hot glue stick (7 mm) | 7 units | R$ 8.05 | Sponge fixation to the mannequin |
| Nylon zipper | 1 unit | R$ 1.50 | To adjust the fabric to the mannequin and enable the replacement of the microbeads |
| Sponge (0.5 cm thick) | 2 sheets (; length: 70 cm; and thickness: 0.5 cm) | R$ 25.50 | Subcutaneous mesh |
| Sponge (0.25 cm thick) | 1 sheet (width; 50 cm; length: 70 cm; and thickness: 0.25 cm) | R$ 10.00 | Subcutaneous mesh |
| Styrofoam microbeads | 1 liter | R$ 8.90 | Subcutaneous tissue |
| Vacuum cleaner | 1 unit | R$ 64.90 | Vacuum suction pump |
| Copperair-conditioning tube þ cylindrical plastic support | 1 unit | R$ 70.00 | Liposuction cannula |
| Fabric: beige mesh | ; length: 150 cm | R$ 15.30 | Skin |
| Fabric: pink mesh | ; length: 150 cm | R$ 5.10 | Skin |
| TOTAL COST (1 model) | - | R$ 261.75 | - |
| COST FOR EACH MATERIAL REPLACEMENT | - | R$ 5.57 | - |

A plastic surgeon, who is a professor and advisor at the LICIP, tested the functionality and compatibility of the model to simulate liposuction. The surgeon approved the simulator and recommended it for the low-cost simulation of the procedure. As the present study did not involve humans or animals, the Research Ethics Committee waived its submis-sion for approval in accordance with the Declaration of Helsinki.
During aspiration, the adapted cannula removed the microbeads and, as the mesh fabric lost the volume repre-senting the adipose tissue, the mannequin acquired a more defined contour, simulating the visual effect of a successful liposuction. The suture of the umbilical region was per-formed separately, enabling the reuse of the model after the incision by replacing the previously-incised sponge with an intact one. As such, the simulator was a practical and efficient tool for training in liposuction techniques.
When available, clinical cannulas and vacuum/liposuction systems can be attached to the simulator. However, to prioritize low cost and reproducibility, the model uses a didactic cannula and an inexpensive negative-pressure source. These materials ensure the learning goals for initial training and expanded access to repetition.
The simulator aims to provide training in specific liposuc-tion tasks: planning entry points, ergonomics/positioning, fan-shaped trajectory and its parallelism, depth/angle con-trol, and cannula/covering tissue handling. It is not intended to faithfully reproduce the haptic properties of tissues (den-sity, resistance, sensitivity), nor to simulate hemostasis or physiological responses.
Results
The synthetic model provided an efficient and inexpensive simulation of the liposuction technique, standing out as a viable alternative for the training of surgical skills. The students had the opportunity to practice the procedure repeatedly in a safe, controlled environment after an extra-curricular theoretical class on the technique.
Due to the model’s body contour and the use of materials simulating specific structures, handling the mannequin and, consequently, completing the simulated liposuction proce-dure was easy. The simulator enabled training in surgical interventions aimed at reshaping the body through incision, aspiration cannula positioning and handling, sutures, and adipose tissue aspiration.
Discussion
The time dedicated to learning surgical skills during medical school is often insufficient.15 This issue mostly arises from the difficulty of applying a financially-accessible, ethically-regulated methodology that enables the successful practice of a given technique. In this context, the use of synthetic models in plastic surgery education has played a critical role in improving medical training by enabling the safe and effective practice of procedures.9
The creation of the synthetic model herein presented represents a central advance within this context, and it is relevant in terms of overcoming the ethical impasse of using fresh cadavers and animal parts for medical skill training.16 The model was accessible regarding material costs and availability when compared to those requiring more ad-vanced technologies, such as three-dimensional (3D) print-ing17 or the use of biological materials, such as postmortem animal flaps18 Moreover, the simulator enabled the replication of the fundamental movements and techniques of liposuction in a safe and controlled manner, with an accept-able level of fidelity. Our model was consistent with the need for educational methods combining cost-effectiveness and efficiency.19
It is worth mentioning the innovation represented by the adaptation of materials, such as using a drilled copper tube and Styrofoam microbeads to simulate the adipose tissue. This creative approach reflects the need for practical and accessible solutions in educational environments.9 The eco-nomic viability of the model makes it especially useful in countries with limited resources allocated to medical train-ing. Despite being a well-established technique, liposuction still presents technical challenges that demand continuous training and refinement of surgeons’ skills.5 Our model addresses precisely this need by enabling students to prac-tice the technique repeatedly and in a controlled manner, improving their skills before transitioning to real-world scenarios.
However, it is crucial to consider that, despite its poten-tial, the synthetic model herein presented has some limi-tations. Liposuction in the clinical practice involves a complex interaction among individual anatomy, surgical techniques, and intraoperative management;20 synthetic models do not reproduce all these aspects. Moreover, there is the slight inconvenience in the fact that the model requires a certain level of skill in sewing and using tools like hot glue during its construction, a feature that tends to be compen-sated for by the potential reuse of the model.
Lastly, the positive test results and the model’s approval by leading plastic surgeons reinforce its efficiency and quality, despite its simplicity and low cost. The precision in simulating real surgical steps and the possibility of reuse increase its value as an educational tool. These aspects corroborate the importance of rigorous training to achieve satisfactory and safe esthetic outcomes.21
Conclusion
Our synthetic liposuction model is inexpensive and repro-ducible, enabling the simulation of the initial stages of the procedure and promoting coordination, ergonomics, and technical familiarization. Its accessibility and repeated prac-tice broaden its reach and democratize surgical training. It is a supplementary educational strategy that contributes to the learner’s training and confidence, without replacing more faithful models or supervised clinical training.
REFERENCES
1. Illouz YG. Body contouring by lipolysis: a 5-year experience with over 3000 cases. Plast Reconstr Surg 1983;72(05):591-597. Doi: 10.1097/00006534-198311000-00001
2. Fournier PF. Liposculpture: The syringe technique. Am J Cosmet Surg 1993;10(03):179-187. Doi: 10.1177/074880689301000305
3. Battisti C, Souza TMd, Possamai LM, Steffen N, Ely PB. Lipoaspi-ração: métodos disponíveis e vantagens da técnica com seringa. Rev Bras Cir Plást 2019;34(Suppl 3):86-88. Doi: 10.5935/2177-1235.2019RBCP0183
4. Gemperli R, Munhoz AM, Marques AdA. Neto. Fundamentos da cirurgia plástica. Rio de Janeiro: Thieme Revinter; 2016
5. Santoro M Júnior, Avelar JM. Cirurgia plástica na infância e na adolescência. Rio de Janeiro: Editora Atheneu; 2018
6. Thorne CH. Grabb & Smith’s: Cirurgia Plástica. Rio de Janeiro: Thieme Revinter; 2018
7. Barros LFL, Teixeira VF, Reis JAP Júnior, Ferraz RA, Araújo DDC, Vendramin FS. Complicações em lipoaspiração: revisão sistemá-tica. Rev Bras Cir Plást 2023;38(01):e0641. Doi: 10.5935/2177-1235.2023RBCP0641-PT
8. Nunes JML, Bonfim ILCB, Alves EHP, Lopes PF. Simulação em educação médica: o ensino da cirurgia. Rev Mult Nord Min 2024;4(01):1-17. Doi: 10.61164/rmnm.v4i1.2344
9. Reznick RK, MacRae H. Teaching surgical skills-changes in the wind. N Engl J Med 2006;355(25):2664-2669. Doi: 10.1056/NEJMra054785
10. Grunwald T, Krummel T, Sherman R. Advanced technologies in plastic surgery: how new innovations can improve our training and practice. Plast Reconstr Surg 2004;114(06):1556-1567. Doi: 10.1097/01.prs.0000138242.60324.1d
11. Valentine R, Padhye V, Wormald PJ. Treinamento de simulação para emergências vasculares em cirurgia endoscópica de seios paranasais e base do crânio. Otolaryngol Clin North Am 2016;49 (03):877-887. Doi: 10.1016/j.otc.2016.02.013
12. Aggarwal R, Darzi A. Technical-skills training in the 21st century. N Engl J Med 2006;355(25):2695-2696. Doi: 10.1056/NEJMe068179
13. Gomes AAR, Soares FVC, Pessoa SGdP. Modelo de treinamento em palatoplastia. Rev Bras Cir Plást 2011;26(04):691-695. Doi: 10.1590/S1983-51752011000400027
14. Dunkin B, Adrales GL, Apelgren K, Mellinger JD. Surgical simula-tion: a current review. Surg Endosc 2007;21(03):357-366. Doi: 10.1007/s00464-006-9072-0
15. Lee MJ, Drake TM, Malik TA, et al. Has the Bachelor of Surgery Left Medical School?-A National Undergraduate Assessment J Surg Educ 2016;73(04):655-659. Doi: 10.1016/j.jsurg.2016.01.005
16. Bezerra PM, Borba MdN, Guerriero ICZ, Dallari SG. Ethical and legal analysis of scientific research on corpses in Brazil. Rev Bioet 2020;28(03):554-564. Doi: 10.1590/1983-80422020283420
17. Lacerda TF, Romanielo AFR, Gomes SdM, et al. Aplicabilidade da impressora 3D na prática médica contemporânea. Braz J Health Rev 2020;3(01):620-625. Doi: 10.34119/bjhrv3n1-050
18. Kinshoku MR, Rodriguez CAL, Fidalgo RdS, Duran CCG, Leme PLS, Duarte IdS. Uso racional de modelos animais para pesquisa e ensino de microcirurgia. Rev Col Bras Cir 2012;39(05):414-417. Doi: 10.1590/S0100-69912012000500013
19. Wu S, Coombs DM, Gurunian R. Liposuction: Concepts, safety, and techniques in body-contouring surgery. Cleve Clin J Med 2020;87 (06):367-375. Doi: 10.3949/ccjm.87a.19097
20. Cárdenas-Camarena L, Reyes-Herrera MF, Vargas-Flores E, López-Fabila DA, Robles-Cervantes JA. Lipoabdominoplasty: What we have implemented and what we have modified over 26 years. Plast Reconstr Surg Glob Open 2023;11(02):e4805. Doi: 10.1097/GOX.0000000000004805
21. Illouz YG. Study of subcutaneous fat. Aesthetic Plast Surg 1990;14(03):165-177. Doi: 10.1007/BF01578345
1. Integrated Medical Care Center (NAMI), Medicine Program, Centro de Ciências da
Saúde,, Universidade de Fortaleza, Fortaleza, CE, Brazil
Address for correspondence Ivens Rafael Resplande de Sá, Núcleo de Atenção Médica Integrada (NAMI), Curso de Medicina, Centro de Ciências da Saúde, Universidade de Fortaleza, Rua Maramaldo Campelo 50, Edson Queiroz, Fortaleza, CE, 60811-640, Brazil (e-mail: ivens1@edu.unifor.br).
Article received: January 26, 2025.
Article accepted: October 13, 2025.
Editor-in-Chief: Dov Charles Goldenberg.
Conflict of Interests
The authors have no conflict of interests to declare.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket