



Case Report - Year 2024 - Volume 39 -
Mondor syndrome associated with breast augmentation: case report
Síndrome de Mondor associada à mamoplastia de aumento: relato de caso
Maria Clara Gomes de Morais1 ; Karley Silva Almeida1; Gabriel Carvalho Fiusa2; Rafael Rodolfo Tomaz de Lima3*; Karla Patrícia Cardoso Amorim1
; Karley Silva Almeida1; Gabriel Carvalho Fiusa2; Rafael Rodolfo Tomaz de Lima3*; Karla Patrícia Cardoso Amorim1
ABSTRACT
The breast form of Mondor syndrome is a rare and self-limited condition characterized by thrombophlebitis of the superficial veins of the breast. Understanding this syndrome is extremely important for correct diagnosis and precise, non-iatrogenic treatment, given that it has a considerable relationship with breast carcinoma. This case report portrays the emergence of Mondor syndrome in a young 22-year-old patient, after breast augmentation. The characteristic sign of the condition, the fibrous cord, appeared in the right breast from the twenty-third day after surgery, disappearing completely after 10 weeks. The diagnosis was given by the plastic surgeon who followed the patient through anamnesis and physical examination, without the urgency of a complementary exam, such as a mammography. It is worth mentioning that this rare condition can affect males - less frequently - and affect other regions, such as the penis and scrotum. Furthermore, it is beneficial to recognize and diagnose Mondor syndrome, as surgeries using phytoaesthetics are constantly growing today, intending to guide patients in the best way possible for an effective and less invasive treatment (except in the concomitant presence of cancer). breast, for example), in addition to reassuring them about the condition.
Keywords: Breast; Thrombophlebitis; Fibrosis; Mammaplasty; Case reports
RESUMO
A forma mamária da síndrome de Mondor é uma afecção rara e autolimitada que se caracteriza pela tromboflebite de veias superficiais da mama. Entender tal síndrome é de suma importância para o diagnóstico correto e o tratamento preciso e não iatrogênico, tendo em vista apresentar considerável relação com o carcinoma mamário. Esse relato de caso retrata o surgimento da síndrome de Mondor em uma paciente jovem de 22 anos, após uma mamoplastia de aumento. O sinal característico da afecção, o cordão fibroso, manifestou-se na mama direita a partir do vigésimo terceiro dia de pós-operatório, desaparecendo por completo após 10 semanas. O diagnóstico foi dado pelo cirurgião plástico que acompanhou a paciente mediante anamnese e exame físico, sem a urgência de um exame complementar, como a mamografia. Vale ressaltar que tal afecção rara pode acometer o sexo masculino - em menor frequência - e afetar outras regiões, como o pênis e o escroto. Ademais, é salutar reconhecer e diagnosticar a síndrome de Mondor, visto que as cirurgias com o fitoestético estão em constante crescimento na atualidade, com o escopo de conduzir os pacientes da melhor forma para um tratamento eficaz e menos invasivo (exceto na presença concomitante de câncer de mama, por exemplo), além de tranquilizá-los a respeito da afecção.
Palavras-chave: Mama; Tromboflebite; Fibrose; Mamoplastia; Relatos de casos
INTRODUCTION
This article aims to report the case of a patient affected by Mondor syndrome in the postoperative period of breast augmentation. Mondor syndrome is a rare, benign, and self-limited condition in which thrombophlebitis occurs in the peripheral venous vessels of the breast, which can even affect the lymphatic system in the region, presenting clinically as a subcutaneous fibrous cord on the anterolateral wall of the chest1.
Thus, the importance of the study is urgent amid the exponential increase in aesthetic surgical interventions in the world, which, in 2019, reached 11,363,569 procedures, a number 7.4% higher than in 2018, according to the International Society of Aesthetic Plastic Surgery ( ISAPS)2. Still according to ISAPS, Brazil, in 2019, was responsible for 13.1% of procedures, totaling almost 1,500,000 interventions2.
Added to this, the relevant association of Mondor syndrome with breast carcinoma requires concern for the disease3. Furthermore, it is essential to properly guide patients affected by this clinical condition, to calm them down, and to treat them appropriately.
CASE REPORT
MCGM, female patient, 22 years old, mixed race, medical student, born in Sousa-PB and from Natal-RN, underwent breast augmentation on 12/05/2020, having progressed uneventfully in the immediate postoperative period.
On the 23rd post-operative day, she began to complain of progressive pain (intensity 5/10) without irradiation in the lower region of the right breast, with the appearance of a thin subcutaneous cord of hardened consistency and high temperature, without factor triggering and improving, which was directed to the upper right quadrant of the abdomen, retracting the skin (Figure 1).
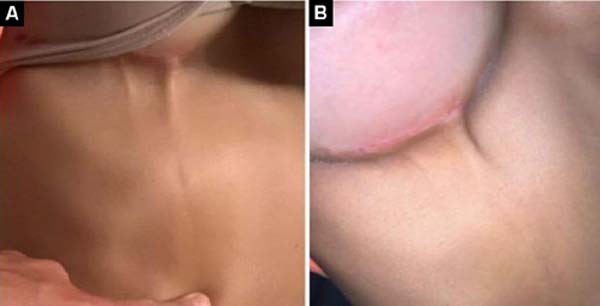

Physical examination confirmed the presence of a fibrous cord that began in the inframammary region and extended to the right upper abdominal quadrant. The plastic surgeon responsible for the aesthetic procedure the patient underwent, through physical examination alone, confirmed the diagnosis of Mondor syndrome.
Afterward, the professional instructed the patient to use Prednisone® 20mg orally once a day, for 7 days, and to apply a warm compress to the area three times a day. Furthermore, he advised the patient about Mondor syndrome, which therefore recognized the self-limited nature of the condition, a situation that reduced the patient’s nervousness and concerns about the syndrome.
There was progressive remission of the fibrous cord projected under the skin, which completely disappeared after 10 weeks, without leaving any scars.
The patient was taking contraceptive therapy without medical advice. In the period of 8 months before the surgery, she was using Iumi®, a combined oral contraceptive.
DISCUSSION
Mondor syndrome is almost ten times more common in women than in men and primarily affects the average age group of 43 years. Presenting greater unilateral involvement, with few reports of bilateral appearance, Mondor syndrome is evident without systemic signs4.
This condition is associated, in up to 12% of cases, with the emergence of breast carcinoma, a situation that explains the concern surrounding its diagnosis3 and makes the need to investigate the disease causing the pathology under discussion imminent.
The etiology related to the development of Mondor syndrome has not yet been completely clarified, with 50 to 60% of cases considered idiopathic5. However, its pathophysiology is similar to deep vein thrombosis (DVT)6 and its genesis is also related to Virchow’s triad (stasis, hypercoagulability, and endothelial damage)7. It is believed that the deficient action of venous valves, by enabling retrograde blood flow, generates stasis that favors the formation of thrombi, which can progress with aggression to the vascular wall and the formation of venous fibrosis typical of the syndrome under discussion8.
The use of oral contraceptives increases the risk of DVT as the dosage of estrogen increases. Estrogen tends to increase levels of clotting factors, reduce levels of antithrombin III, and decrease plasminogen activator9. Some risk factors are associated with the development of the disease, such as surgical procedures, breast cancer, trauma, injectable drug abuse, pendulous breasts, excessive physical activity, pregnancy, blood dyscrasia, infections, and rheumatoid arthritis9.
The characteristic lesion of Mondor syndrome begins with the appearance of a rounded, painful, reddish cord, which progresses to a thick, painless fibrous line10, whose structure becomes more evident with the abduction movement of the arm. The appearance of the fibrous cord is limited, preferably, to the inframammary region, with its appearance until the fourth week after surgery and total remission until the eighth week4.
A priori, the clinical condition of patients with Mondor syndrome is characterized by pain, increased breast volume, and retraction of the skin at the level of the lesion, which can be identified as a fibrous cord or palpable mass on physical examination. Furthermore, the patient may be asymptomatic or even have less common symptoms, such as fever, bruising, and skin inflammation5.
A mammogram is an exam that can be requested, observing a tubular, dilated, long, and superficial density, giving a “rosary bead” appearance, thus suggesting thrombosis of the affected vein4. The importance of this examination is mainly due to the possibility of diagnosing non-palpable breast neoplasia.
Treatment for Mondor syndrome is symptomatic only. Generally, a warm compress is used at the site of thrombophlebitis and rest and the use of analgesics and non-steroidal anti-inflammatory drugs are recommended. For the doctor and examiner, it is essential to inform the patient about the benign and self-limited nature of the condition, accepting their concerns.
CONCLUSION
In light of these considerations, it is concluded that Mondor syndrome is a rare condition and its main characteristic is the presence of a fibrous cord caused by the formation of a thrombus, with the breast being the most affected region of the human body - emerging as a complication breast surgery, but it can also affect males to a lesser extent, preferably affecting regions of the penis and scrotum.
Finally, it is worth highlighting that it is a benign and self-limited condition (with a beginning, middle, and end), but that, due to its relationship with breast carcinoma, it requires attention for its diagnosis.
REFERENCES
1. Faucz RA, Hidalgo RT, Faucz RS. Doença de Mondor: achados mamográficos e ultra-sonográficos. Radiol Bras. 2005;38(2):153-5.
2. International Society of Aesthetic Plastic Surgery (ISAPS). International Survey of Aesthetic/Cosmetic Procedures 2019. Mount Royal: ISAPS; 2019.
3. Catania S, Zurrida S, Veronesi P Galimberti V, Bono A, Pluchinotta A. Mondor’s disease and breast cancer. Cancer. 1992;69(9):2267-70.
4. Becker L, McCurdy LI, Taves DH. Superficial thrombophlebitis of the breast (Mondor’s disease). Can Assoc Radiol J. 2001;52(3):193-5.
5. Pasta V D’Orazi V Sottile D, Del Vecchio L, Panunzi A, Urciuoli P. Breast Mondor’s disease: Diagnosis and management of six new cases of this underestimated pathology. Phlebology. 2015;30(8):564-8.
6. Sobreira ML, Yoshida WB, Lastória S. Tromboflebite superficial: epidemiologia, fisiopatologia, diagnóstico e tratamento. J Vasc Bras. 2008;7(2):131-43.
7. Alvarez-Garrido H, Garrido-Ríos AA, Sanz-Muñoz C, Miranda-Romero A. Mondor’s disease. Clin Exp Dermatol. 2009;34(7):753-6.
8. Khan UD. Incidence of mondor disease in breast augmentation: a retrospective study of 2052 breasts using inframammary incision. Plast Reconstr Surg. 2008;122(2):88e-89e.
9. Favarin GJ, Favarin E, Rocha LPS, Horner C. Mondor’s disease, case report and literature review. Arq Catarin Med. 2016;45(2):102-6.
10. Piccinato CE. Trombose venosa pós-operatória. Medicina (Ribeirão Preto). 2008;41(4):477-86.
1. Universidade Federal do Rio Grande do Norte, Natal, RN, Brazil
2. Universidade de Brasília, Brasília, DF, Brazil
3. Secretaria de Estado da Saúde Pública, Centro Estadual de Reabilitação e Atenção Ambulatorial Especializada, Natal, RN, Brazil
Corresponding author: Rafael Rodolfo Tomaz de Lima Av. Alexandrino de Alencar, 1900, Tirol, Natal, RN, Brazil. Zip Code: 59030-660, E-mail: limarrt@gmail.com
Article received: September 18, 2023.
Article accepted: April 30, 2024.
Conflicts of interest: none.
Institution: Universidade Federal do Rio Grande do Norte, Natal, RN, Brazil.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket